In praise of ‘big data’ and analysis – putting a value on prevention
By: Professor Les Mayhew, ILC
Following our year-long Prevention in an ageing world programme that sparked conversations from Abu Dhabi to Taipei, Austin, Geneva, Sydney, London all the way to the G20 Health Ministers, the message is clear. It’s never too late to prevent.
Last year we highlighted how the health and economic costs of failing to invest in preventative interventions across the life course are simply too high to ignore.
But whilst Governments and healthcare professionals seem to agree that prevention is better than cure, can we get better at putting a price a on it? And how can we use this evidence to deliver action to tackle health inequalities and engage policymakers and healthcare workers.
Using big data to put a financial value on prevention could transform our decision making and improve our allocation of scarce resources, improve health and save the NHS money. Long considered the holy grail of public health, progress on this front has been faltering at best.
It turns out that a lot of public health’s achievements become apparent with the passage of time through advancements in life expectancy. Such advances are the net effect of many different factors and are hard to attribute. Nevertheless, the lessons learnt are not lost because they are transferrable to other communities and generations. When that effect is positive we celebrate but we are often unable to disentangle cause and effect and therefore costs from savings – at least until well after the event. The COVID crisis has brought this into much sharper focus simply because the people most at risk of hospitalisation and death have pre-existing conditions, which are often preventable.
A recent study in East London, in one of the most deprived areas of the country, has made modest but real progress in this regard. Using the anonymised medical records of all residents –some 300,000 – to linked council datasets including housing and welfare benefits, it was able to demonstrate clear links between deprivation and life styles on the one hand, and hospital admission costs, out patient attendance and visits to A&E on the other. Type 2 diabetes, a key COVID risk factor, is a lifelong condition that can affect your everyday life and can also increase your risk of getting serious problems with your eyes, heart and nerves. One of the many case studies undertaken looked at the prevalence of diabetes in the population and links to modifiable risk factors such as obesity, smoking habits and others. Hypertension or high blood pressure turns out to be one of the main risk factors which are easily preventable by eating healthily, maintaining a healthy weight, engaging in regular exercise, drinking alcohol in moderation and not smoking.
Based on 230,000 adults aged 20-64, the study found that 5% of residents had been diagnosed with diabetes but that this varied according to the number of risk factors in a person. It found for example that of the 1,500 residents -or just under 1% of the total- who were hypertensive, obese and male, 41% were diabetic. For 25% of the population with none of these risk factors, diabetic prevalence dropped to only 2.4% in this sub-group. The analysis went on to show that susceptibility to diabetes increased 2.3 times in obese people, 12.5 times in hypertensives, 1.5 times in current or ex-smokers and 1.15 times in males. These risks are multiplicative so a person in all four risk categories was 54 times higher as compared with someone with no risk factors. Statistically, these four risk factors – all of which are statistically significant and modifiable apart from gender – explained 90% of prevalence variation based on all possible risk factor combinations.
So what, you might say! If attention is turned to secondary care services i.e. inpatients, outpatients and A&E attendances, we see how quickly interaction with health services is escalated as a result. Since each spell in hospital or outpatient attendance or A&E visit is subject to a tariff, the study is also able to put a cost on each risk factor singly or in combination. For example it finds that during the year, those in the highest risk category are five times more likely to experience a hospital spell for any reason on average than a person with no risk factors and that the secondary care costs per patient per year are between 7 and 9 times higher. Figure 1 shows the overall effect on inpatient spells and secondary care costs which are estimated using multiple regression. The risk factors are split into five categories – obesity, current or ex-smoker, diabetes and hypertension. If no risk factors are present, then the baseline cost in this age group is only £155. However, costs escalate by £469 if a person is diabetic, £382 if hypertensive, £237 if a current or ex smoker and by £225 if obese. Note that the costs are additive and also averages so that individual cases might be much higher or lower.
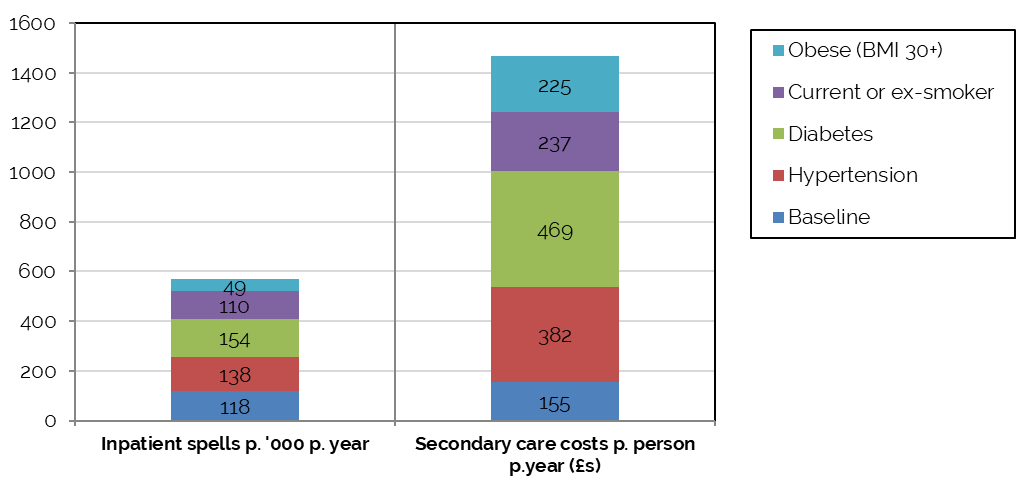
Figure 1: Inpatients spells and the cost of secondary care by risk factor
The clear implication, however, is that much money could be saved for the NHS if these risk factors could be eliminated, if people took greater care of their health and diet and were helped to do so by the appropriate advice and polices. How robust are these findings? Figure 2 shows the predicted versus observed secondary care costs per person – the model statistically explains 93% of the variation and is therefore, predictively speaking, pretty good.
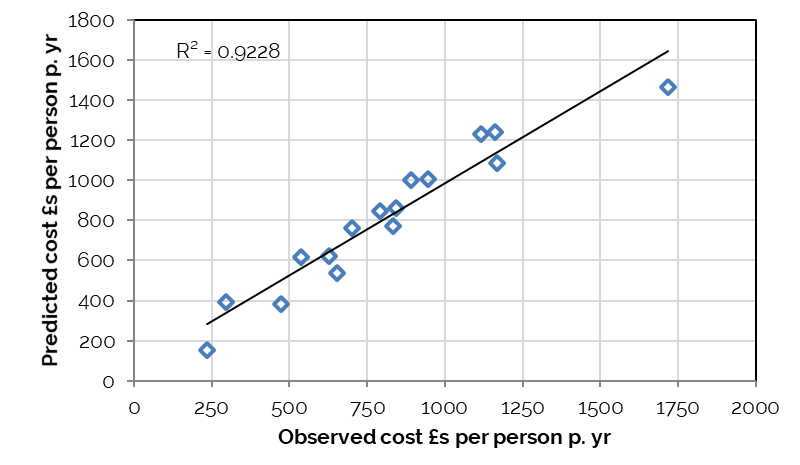
Figure 2: Predicted versus observed secondary care costs based on the risk factors in Figure 1
As illustration of the implications of these findings, compare the same adult population with none of these risk factors with the current population. The current cost of secondary care for this adult group is £78m a year but if none of these risk factors were present, the cost would fall to £55m assuming the same level of interaction with the health service. However, this is a conservative estimate since a healthier population would be expected to use the same services less than previously, in which case the indicated savings of £23m a year would be much higher.
It is also worth noting that the analysis pre-dates the COVID-19 epidemic by over a year and so if it was repeated today, we believe the effects of any of these risk factors are likely to be much greater. These are not trivial sums, nor are they easy to realise but they do show the importance of good health and the value of prevention versus the alternative of spending ever greater amounts of money on healthcare for preventable conditions. They are not the complete story of course since people without these risk factors would be healthier and more able for example to work, train or volunteer i.e. the wider benefits would potentially far outweigh the costs.
ILC is working to follow up on our “Prevention in an ageing world” programme by exploring not only “why” we ought to prioritise prevention across the life course but “how” we can deliver it. We will be exploring how we can:
- Democratise access to prevention – to reduce health inequalities
- Inspire and engaging policymakers, healthcare professionals and individuals – to invest, promote and take action on prevention
- Effectively utilising technology – to improve access to health care, improve uptake rates, reduce barriers and empower patients.
The effective use of big data could help us tackle inequalities in health as well as better engage policymakers and health care professionals with the importance of preventing ill health. We will be launching a series of consultation papers, which will explore how we can deliver prevention across the world. Keep an eye on our website for more information.
Professor Les Mayhew
Global Head of Research, ILC
Les joined ILC in October 2020 as Head of Global Research and will be working on a range of ILC research projects as well as enhancing our research approach and strategy.
Les is also part-time Professor of Statistics at The Business School (formerly Cass), City University, London, and Managing Director of Mayhew Harper Associates Ltd. His previous experience includes 20 years in the Department of Health and Social Security, the Department of Social Security, HM Treasury and the Office for National Statistics, where he was a director. He is an alumnus of the International Institute for Applied Systems Analysis (IIASA), Vienna, an Honorary Fellow of the Institute of Actuaries, and a member of the Royal Economic Society.